Why Baseline Recruitment Sets the Retention Foundation
Baseline patient recruitment is not just about filling study slots; it sets the quality of the participant cohort and the operational tone that directly underpins long‑term retention in clinical trial services. When you recruit the right patients at the outset, those who are eligible, motivated, and logistically aligned you build a stable cohort that is far more likely to stay engaged through visits, follow‑ups, and protocol complexities.
Right‑fit participants
Clear, well‑defined eligibility criteria and thoughtful screening at baseline ensure that enrolled patients genuinely match the trial’s medical and lifestyle requirements. This reduces protocol violations, safety‑related exits, and disenchantment later in the clinical study, which are common drivers of dropout.
Informed expectations from day one
A robust recruitment process includes transparent communication about visit frequency, procedures, and time commitments. When patients enter the clinical trial with realistic expectations, they are less likely to withdraw due to perceived burden or logistical strain.
Foundation of trust and engagement
Early interaction, during recruitment and consent shape patients’ perceptions of the research team and the sponsor. When staff listen to concerns, respect patient preferences, and explain the “why” behind the trial, they lay a trust‑based foundation that increases willingness to remain in the study.
Feasibility‑driven protocol design
A strong baseline recruitment strategy is informed by real‑world data on site capacity, patient travel patterns, and local disease burden. This forces the team to design protocols that are logistically feasible for the enrolled population, minimizing no‑shows and unscheduled dropouts.
Diversity and representativeness
Inclusive, targeted recruitment at baseline improves demographic and clinical diversity, which in turn enhances engagement across subgroups. Participants who see themselves reflected in the trial population are more likely to feel valued and invested in the research outcomes.
Optimizing Screening for Long Term Commitment
Optimizing screening processes ensures participants demonstrate sustained dedication, minimizing dropouts in extended studies. This is vital in clinical trials where long term adherence impacts data quality and outcomes.
Define Clear Criteria
Establish upfront metrics for commitment, such as prior trial participation history, availability for follow-ups, and willingness to use digital tools for virtual clinical trial monitoring. These reduce early attrition by 20-30% in decentralized trials. Tailor criteria to trial demands, prioritizing reliability over volume.
Leverage Behavioral Assessments
Use validated questionnaires to gauge motivation and resilience, like those assessing patient-reported outcomes on adherence intent. Incorporate short simulations of trial protocols to predict follow-through. This identifies high commitment candidates early, enhancing retention.
Implement Tiered Screening
Start with quick digital pre screens (e.g., app based eligibility quizzes), followed by video and probing long term feasibility. Finalize with a probationary engagement period tracking engagement metrics. Tiering streamlines volume while focusing on sustained fit.
Utilize Predictive Analytics
Apply AI-driven risk models to score participants based on demographics, past behavior, and linked to retention. Models from pharmacovigilance data can flag dropout risks with 85% accuracy. Regularly refine algorithms with trial data for precision.
Personalization from Day One: The Recruitment and Retention Link
In decentralized clinical trials (DCTs), recruitment isn’t just about filling slots it lays the groundwork for long term retention. The patient diversity, digital access, and healthcare expectations vary widely, data driven recruitment helps sponsors align participants with trial demands from day one. By considering demographics, digital literacy, and personalized incentives, sponsors can build engagement even before the first virtual visit.
Consider a mid sized oncology DCT targeting 500 patients. Traditional recruitment models often experience 30–40% dropout rates due to mismatched expectations and access barriers. Instead, AI powered platforms can optimize participant matching by analyzing:
- Demographics: Match patients based on age, geography (e.g., urban New York vs. rural Midwest), comorbidities, and cultural factors. For example, a 50 year old tech savvy professional in California may prefer a fully remote, app based trial, while an older patient in a rural setting may require hybrid support with local healthcare providers.
- Tech Comfort: Use short digital assessments or integrated health apps to evaluate familiarity with eConsent, wearables, and ePRO tools. Digitally confident participants can move through fully remote workflows, while others benefit from onboarding support, simplified interfaces, or alternative participation methods.
- Incentives: Personalize engagement strategies using predictive analytics, financial stipends for cost sensitive participants, wellness focused rewards for health conscious individuals, or early access to study insights for research motivated patients. Studies indicate that tailored incentives can improve enrollment by up to 25% and retention by 35% in DCT environments.
This approach builds trust early participants feel understood rather than generalized. In similar USA based DCT implementations, personalized recruitment strategies have reduced early dropouts by nearly 30% and improved patient satisfaction by over 40%.
The outcome is clear: stronger retention, higher quality data, accelerated timelines, and reduced operational costs proving that in decentralized trials, personalized recruitment is a critical driver of long term success.
Tech Enabled Patient Retention Strategies for Seamless Onboarding
In hybrid clinical trials, where participants blend in person and remote elements, early attrition often stems from cumbersome onboarding processes like paperwork delays, forgotten appointments, and low engagement. Integrating virtual platforms such as eConsent and app based reminders addresses these pain points, streamlining recruitment and fostering retention from day one.
Key Implementation Steps:
-
eConsent Platforms: Deploy digital consent tools (e.g., Compliancy Group or Medidata Rave eConsent) that allow multimedia explanations, interactive Q&A, and real time signatures via mobile devices. Participants review materials at their pace, reducing confusion and dropout rates by up to 30% (per recent DCT benchmarks).
-
App Based Reminders and Check-Ins: Use patient apps like those from Medable or Science 37 to send personalized nudges for trial milestones. e.g., “Complete your baseline survey in 2 minutes” or “Your virtual onboarding session starts in 1 hour.” Gamification elements, such as progress badges, boost engagement.
-
Integrated Onboarding Flow: Link eConsent directly to trial apps for seamless progression: consent → profile setup → virtual orientation → first data entry. AI driven personalization tailors reminders based on user behavior, ensuring high completion rates.
Expected Outcomes:
This approach cuts onboarding time from weeks to days, minimizes no shows by 25-40% (as seen in virtual trial pilots), and enhances diversity by overcoming geographic barriers. For pharmacovigilance, it also enables early safety signal capture through embedded PRO modules.
In practice, a Phase III oncology hybrid clinical trial using these tools reported 92% onboarding
How to use Patient Retention Strategies Data to Refine Recruitment
Patient retention data can be a powerful lever to refine patient recruitment by exposing which patients are most likely to stay enrolled and why they leave, so recruitment can be pre‑targeted toward “high‑stay” profiles and away from high‑risk profiles. Below is a structured content outline you can use or adapt for a talk, slide deck, or SOP style guidance.
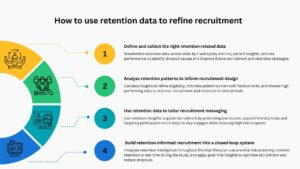
Step 1: Define and collect the right retention‑related data
To use retention data effectively, standardize what you capture across trials:
Core metrics
-
Screen‑fail rate, consent‑to‑randomization rate, dropout rate by visit/window, and reasons for withdrawal (e.g., AE, burden, travel, lack of efficacy perception)
-
Time‑to‑dropout by site, geography, and demographic strata (age, gender, comorbidities, socioeconomic factors).
Patient‑reported drivers
Post‑exit surveys, in‑trial feedback, and site‑level qualitative notes on “why patients left” can highlight burden‑related issues (visit frequency, travel, paperwork, communication gaps).
Site‑level performance
Enrollment speed vs. retention per site; sites with high recruitment but low retention often signal workflow or communication problems that should feed into future site selection and training
Step 2: Analyze retention patterns to inform recruitment design
Use the data to shape your next trial’s recruitment strategy:
Refine eligibility criteria
Refining eligibility criteria helps improve patient retention in clinical trials. If patients with comorbidities or mobility challenges tend to drop out, criteria can be adjusted or supported with services like transport or home visits. Excluding highly complex cases may slow enrollment but can reduce overall attrition.
Adjust burden and visit structure
If dropouts occur due to frequent lab or clinic visits, reduce visit frequency, shift some to telehealth, and enable home based data collection. Promoting this “lighter” design as fewer in clinic visits can improve recruitment and retention.
Optimize site selection and site support
To optimize site selection and support, sponsors should use historical retention data to prioritize high performing sites and avoid those with frequent dropouts. Training site staff on past dropout causes such as poor communication and inflexible scheduling can improve patient retention, ensure consistent messaging, and enhance overall trial outcomes.
Step 3: Use retention data to tailor recruitment messaging
Retention‑driven insights can be turned into concrete recruitment messages:
Highlight “de‑risked” aspects of the clinical trial
Highlighting “de-risked” elements like remote monitoring, flexible visit windows, and transportation support can boost patient confidence and enrollment. Using messages such as “Designed with fewer clinic visits based on participant feedback” shows the study is patient-centric and built on past insights, making participation easier and more appealing.
Segment recruitment by retention‑prone profiles
Segmenting recruitment by retention prone profiles helps improve trial outcomes. Target patients more likely to stay engaged, such as employed individuals with telehealth access or those in urban areas through focused digital campaigns. Simultaneously, avoid over recruiting high risk groups like frequent travelers unless additional support is provided to ensure retention.
Step 4: Build retention‑informed recruitment into a closed‑loop system
Embed retention learning into the trial lifecycle:
Pre trial
Use a “retention‑risk checklist” derived from historical data when designing recruitment and retention plans; explicitly link high‑attrition points to recruitment tactics (e.g., pre‑screening for travel access).
During trial
Monitor real‑time retention metrics (e.g., first‑visit completion rate, missed‑visit frequency) and quickly adjust recruitment: pause or redirect campaigns if early signals suggest a repeat of prior dropout patterns.
Post trial
Feed attrition reasons and high‑retention profiles into a centralized database so future protocols automatically “inherit” optimized recruitment criteria and messaging.
Final Thoughts
Optimizing baseline recruitment is no longer just a starting point, it is a strategic lever that shapes the entire trajectory of a clinical trial. From selecting the right fit participants to leveraging data driven screening, personalization, and technology enabled onboarding, every early decision directly influences long term retention, data quality, and clinical study success.
By integrating retention insights into recruitment planning, sponsors can move from reactive problem solving to proactive trial design targeting participants who are not only eligible but also engaged and committed. The shift toward a closed loop, retention informed recruitment model ensures continuous learning, smarter site selection, and more patient-centric protocols.
Ultimately, trials that prioritize alignment between patient needs, protocol feasibility, and digital enablement from day one are better positioned to reduce attrition, accelerate timelines, and deliver reliable outcomes. In an increasingly competitive and decentralized clinical research landscape, recruitment and retention are no longer separate functions they are deeply interconnected pillars of clinical trial excellence.